
Clinical History :
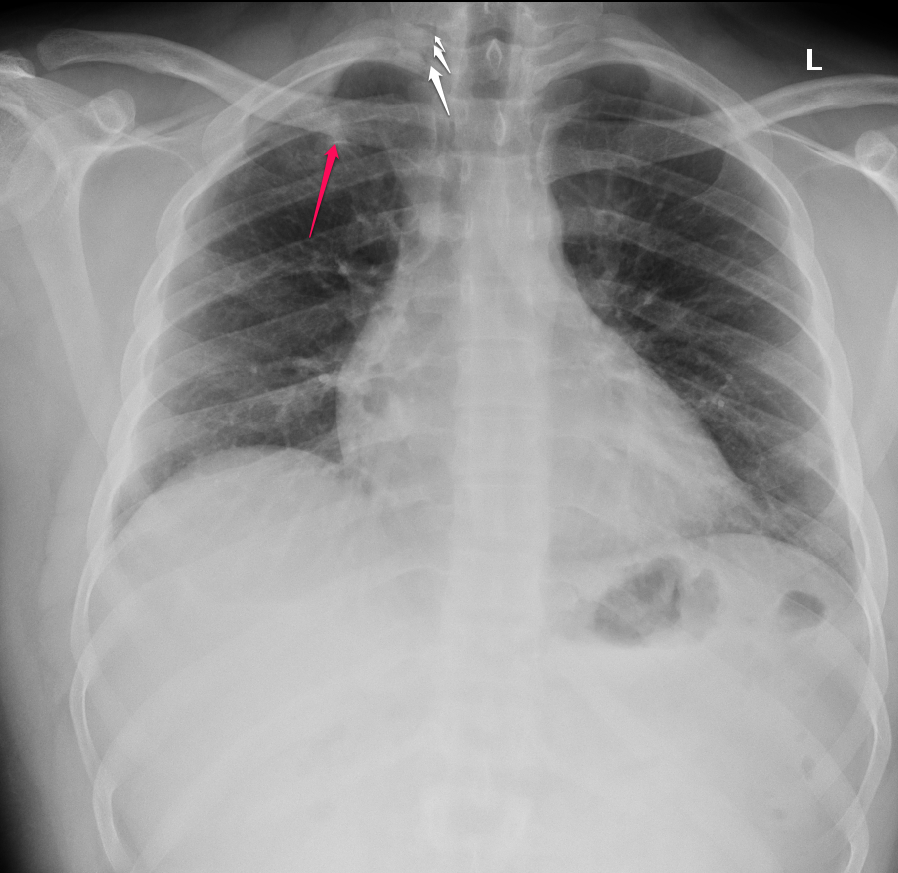
19 years old male patient with history of SOB.

------------------------------------------------------------------------------------------------
Findings:

There is a faint left lower lobe retrocardiac opacity (red arrows) associated left plural effusion ( yellow arrow).
Left pigtail (blue arrow).
------------------------------------------------------------------------------------------------
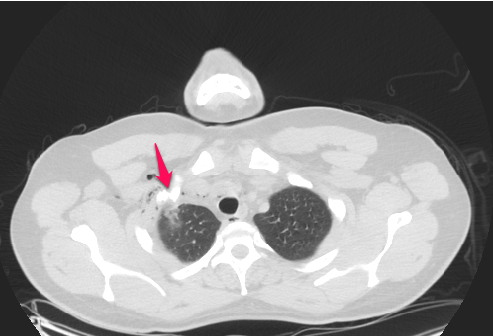
Enhanced chest CT scan was performed




------------------------------------------------------------------------------------------------
FINDINGS




There is tabulated highly vascularized left para-spinal mass( red arrow) showing heterogeneous peripheral enhancement with necrosis and a focus of calcification centrally ( blue arrow). There is large feeding vessels ( green arrow) connecting to a very large aneurysmally dilated para-spinal vessel ( orange and white arrows). No intraspinal extension.
--------------------------------------------------------------------------------------------------------------
Final diagnosis :
Neuroendocrine tumor.












{kind=link}